SummaryWhite matter hyperintensities (WMH) are important markers of cerebrovascular burden that can influence cognitive impairment and Alzheimer's disease progression, with implications for improving patient stratification in clinical trials. Our study uses AI-enabled MRI analysis to quantify WMH and explores their role alongside amyloid status and other biological profiles in predicting cognitive impairment. We found:
|
As Alzheimer’s disease trials become more biologically targeted, understanding patient heterogeneity is increasingly important. Amyloid accumulation, hippocampal atrophy, vascular disease and genetic risk can all shape cognitive trajectories, yet cerebrovascular burden remains under-characterised in many modern trials.
White matter hyperintensities (WMH) are one visible marker of that burden. At IXICO, we used automated, AI-enabled MRI analysis to quantify WMH measures, including lesion burden and confluence, and ask whether they can support more precise patient stratification, reduce noise in trial populations and improve sensitivity in anti-amyloid trials.
What are white matter hyperintensities, and why do they matter in Alzheimer’s disease?
White Matter Hyperintensities (known as WMH) — also referred to as lesions — appear as bright regions on FLAIR MRI scans. They are commonly interpreted as markers of small vessel disease, a form of vascular injury that affects the brain’s white matter. In Alzheimer’s disease, WMH matter for two reasons. First, they may contribute to cognitive impairment independently of amyloid or tau pathology. Second, they can influence eligibility for anti-amyloid treatment trials because substantial white matter burden may increase concern around amyloid-related imaging abnormalities, known as ARIA.
Our study used data from a cohort from the Alzheimer’s Disease Neuroimaging Initiative (ADNI), a large longitudinal dataset that includes brain imaging and clinical information from cognitively normal older adults, people with mild cognitive impairment and people with Alzheimer’s disease.
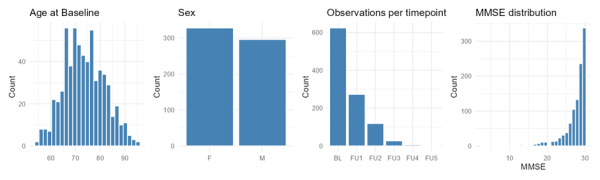
Age, gender balance, distribution of visit time points, and the distribution of cognitive scores (MMSE) in the cohort of participants we analysed.
AI-enabled segmentation of WMH
Using these data, our team segmented WMH using our in-house deep learning tool (one of our volumetric MRI imaging biomarkers analysis tools), then extracted measures such as volume, count, and location.
We calculated all measures across the whole brain and within specific compartments. As findings were broadly consistent across both approaches, we focus here on the whole brain measures.
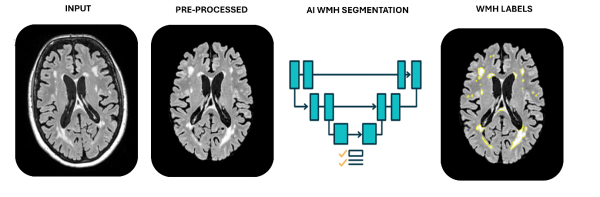
Segmenting WMH using IXICO’s in-house deep learning tool. The yellow highlighted regions show the segmented WMH.
Do WMH predict cognitive impairment?
Yes, white matter hyperintensities are associated with cognitive impairment, but before getting into the results, a note on the statistical approach and the methodology used to avoid inappropriate assumptions in the data.
The cognitive scores in our cohort were highly skewed because many participants scored close to “perfect” on the Mini-Mental State Examination (MMSE), indicating relatively preserved cognition . This violates the assumptions required for standard linear regression methods, so we transformed the data into a reversed proportion, meaning a score of zero no indicated “perfect” cognition, and a score of one indicated the most impairment measurable. With the data transformed this way we were able to use a zero-inflated regression instead.
After controlling for age, sex and hippocampal volume, this statistical model was able to answer two questions at once: does WMH burden predict the chance of being impaired? And, among those already impaired, does WMH burden predict how severe that impairment is?
It also included an interaction with time, asking whether higher lesion burden predicted faster worsening at subsequent follow-up visits.
The results suggest that WMH burden is linked to the onset of impairment. Participants with higher lesion burden were more likely to be impaired, and the burden-by-time interaction suggested that higher lesion burden increased the chance of becoming impaired over time.
The severity model tells a more nuanced story. Among participants who were already impaired, lesion burden was associated with worse impairment, but it did not accelerate decline beyond the effect of time.
In summary, our results indicate that WMH burden is associated with the onset and severity of cognitive impairment, but not with faster worsening of severity over time.
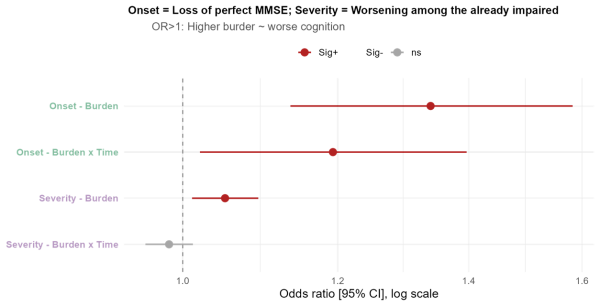
Effect sizes for the Onset (green) and Severity (purple) analyses. Horizontal line crossing 1.0 on the x-axis (dotted line) indicates no significant effect.
Does amyloid status change the relationship between WMH and cognitive decline?
Our previous result raises the question of why WMH burden does not appear to accelerate decline among those who are already impaired. One explanation could be that these participants already have more advanced Alzheimer’s pathology, which may be the dominant driver of deterioration in cognitive state.
To explore this, we split our cohort by amyloid status: amyloid-positive, indicating higher Alzheimer's pathology, and amyloid-negative, indicating lower Alzheimer’s pathology. We then examined the relationship between lesion burden and cognitive decline separately in the two groups.
Our results showed that lesion burden, measured as overall volume, was significant as a marker of cognitive decline only in the amyloid-negative cohort. In other words, when amyloid is low, WMH appear to be a significant contributor to cognitive decline. When amyloid is high, lesions do not appear to play a significant additional role in cognitive decline, irrespective of time.
This is where the WMH confluence measure becomes important. As a reminder, higher lesion confluence indicates that multiple lesions have merged and may be a proxy for more advanced disease.
When we examined confluence in amyloid-positive participants, we found an interaction with time: higher lesion confluence was associated with a faster rate of decline, even after accounting for total lesion volume.
Together these results suggest that when amyloid levels are low, overall lesion volume plays a significant role in cognitive impairment. When amyloid levels are high, patients with more established WMH pathology, indexed by lesion confluence, deteriorate faster.
Interpretation-wise, this just gives us a statistical and measurable method of stating the obvious; that in patients with more advanced Alzheimer’s pathology, cognitive scores are worse. It also suggests that the size and merging of lesions may provide information that total burden alone misses - and should be considered in trial measurements.
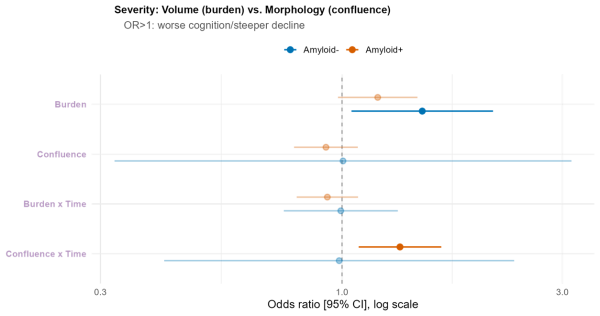
Effect sizes for the Onset (green) and Severity (purple) analyses. Horizontal line crossing 1.0 on the x-axis (dotted line) indicates no significant effect.
Can biological profiles improve Alzheimer’s patient stratification and predict cognitive decline?
Next, we wanted to see whether combining multiple biological indicators could help profile each person, and whether any profile was more predictive of cognitive decline.
First, we used non-negative matrix factorisation, or NMF, to ask whether combinations of disease markers could define meaningful patient profiles. This model included lesion burden across 10 different brain regions, lesion confluence, amyloid status measured via centiloid, hippocampal atrophy and genetic risk via APOE status.
NMF is an unsupervised method, meaning it groups patterns in the biological data without using cognitive scores to create those groups. It identified three main profiles: a genetic risk profile, a WMH burden profile and an atrophy profile.
Individual patients were not forced into a single category. Each person received a score for every profile, allowing the analysis to capture mixed pathology within the same individual. Clinically, that is important because two people with the same diagnosis may have different underlying drivers of cognitive impairment.

NMF identified three profiles. Genetic risk (profile 1), WMH burden (profile 2), and atrophy (profile 3). Note that while centiloid level loads most strongly on profile 1, it also loads onto profile 3, providing a link between the two Alzheimer’s Disease-driven profiles. Additionally, while confluence loads strongly onto profile 2, it is also a driver of profile 3, reinforcing it as potential marker of more advanced pathology.
The second step was to cross-reference the profiles with cognitive impairment and their interaction with time.
We first examined the relationship between the three profiles and the likelihood of cognitive impairment. All three profiles were significantly associated with the probability of being impaired. However, none showed a significant interaction with time. Regardless of how strongly an individual expressed any of these profiles, the model predicted whether they were impaired, but not how quickly they transitioned from an unimpaired to an impaired state over time.
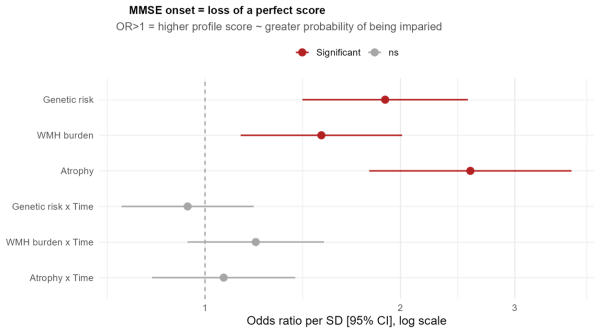
Effect sizes for the Onset analysis examining the contribution of different NMF profiles to cognitive impairment. Horizontal line crossing 1.0 on the x-axis (dotted line) indicates no significant effect.
We then focused on participants who were already impaired to assess whether the profiles were associated with disease severity and progression. The white matter hyperintensity (WMH) profile showed only a weak association, reaching borderline statistical significance. In contrast, both Alzheimer’s pathology profiles — genetic risk and atrophy — were strong predictors of baseline impairment severity. They also showed significant interactions with time, indicating that higher levels of Alzheimer’s-related pathology were associated with both greater impairment and a faster rate of decline over time.
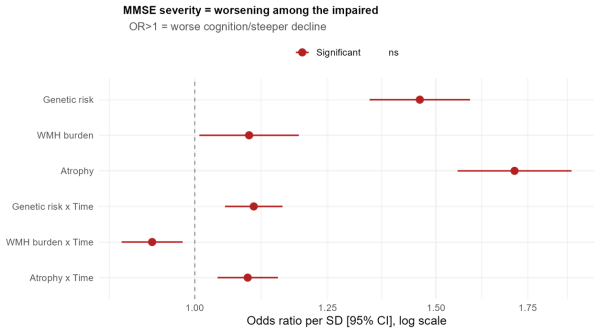
Effect sizes for the Severity analysis examining the contribution of different NMF profiles to cognitive impairment. Horizontal line crossing 1.0 on the x-axis (dotted line) indicates no significant effect.
Together, these findings reinforce the value of stratification. Instead of treating Alzheimer’s disease as a single pathway, we can use imaging and biomarker profiles to separate participants whose decline may be driven by different biological mechanisms.
How can WMH scores support anti-amyloid trials?
Fundamentally, these findings provide valuable insight that excluding participants with high WMH burden may help improve the sensitivity of anti-amyloid trials.
Why? Because in these trials, a key outcome measure for drug efficacy is often related to cognitive score and the slope of decline over time, and the margins can be small. The complex nature of the relationship between WMH and cognitive impairment adds statistical noise to analyses designed to measure the efficacy of candidate treatments. In essence, excluding patients with high WHM can reduce this statistical noise, making it easier to detect subtle treatment effects. We ran simulations which show exactly this.
Moving forward, our data provide a strong rationale for more refined WMH measures, including differentiating between lesion confluence and lesion burden. NMF profiles could also provide insight for better trial design by showing how vascular injury overlaps with amyloid, atrophy and genetic risk.
That distinction is especially relevant because clinical trial populations are heterogeneous. One subgroup may be driven mainly by Alzheimer’s-related genetic risk, another by established atrophy, and another by vascular or white matter pathology. These groups may decline at different rates and may respond differently to a given intervention.
Better stratification could help sponsors select participants, interpret trial outcomes and design studies that are more closely matched to a therapy’s mechanism of action. For participants with early cognitive decline, high WMH burden and less evidence of Alzheimer’s-related atrophy or genetic risk, our findings suggest that a vascular or white matter-focused strategy may be more appropriate than assuming a typical Alzheimer’s disease trajectory.
In summary: Can WMH act as a cerebrovascular biomarker to support Alzheimer's clinical trial design?
Yes, consideration of WMH may help us move toward more precise Alzheimer’s trial design. WMH burden appears relevant to the onset of cognitive impairment, confluence may add prognostic information in amyloid-positive participants, and biological profiles may help explain why people with similar clinical diagnoses follow different paths. Taken together, these measures could support safer enrolment decisions, clearer trial populations and more informative patient stratification.
|
We are a recognised leader in volumetric MRI analysis including WMH. Our automated analysis accurately quantifies the volume of WMH across five different regions and forms part of our neuroimaging biomarkers focus using IXI™. Find out how our IXI™ platform can support your trial. |